Steven, the VP operations of a media company, was asked to present on the organization’s digital transformation program to its top 100 executives during an annual strategy retreat. As public presentations had never been his forte, Steven spent an extraordinary amount of time preparing for the event. But despite these preparations, he blanked out when it was his turn to speak. His presentation was so bumbling and confused that Steven couldn’t bear to go into work the next day…or the next one after that. The complex set of emotions that Steven was feeling have a simple name: shame.
Given the way we react to shame, it shouldn’t come as a surprise that the roots of the word derive from an older Proto-Indo-European word meaning “to cover.” To feel ashamed brings up associations of wanting to hide our faces behind our hands, desperate desiring to run away, or even hoping the earth will swallow us up. At the heart of feeling ashamed is a feeling that we are exposed — either to others or to ourselves. No other feeling is more disturbing or destructive to the self.
After a major mistake, it’s natural to feel ashamed. And yet calling in sick like Steven did is not the answer. Instead, you need to understand the feeling and find a way to let it go.
Down the Rabbit Hole
People who pathologically feel shame tend to internalize and overpersonalize everything that happens to them. They cannot see things in perspective. When something goes wrong, they say to themselves, “I’m to blame for what happened. It’s entirely my fault.” Not only do they demean themselves, but they also feel helpless, and don’t think that there’s anything they can do to change the situation. The internal critic in their heads continually judges and criticizes them, telling them that they are inadequate, inferior, or worthless.
This can have a profound effect on our psychological well-being. Excessive feelings of shame are at the heart of much psychopathology. It is concealed behind guilt; it lurks behind anger; it can be disguised as despair and depression. As people rarely talk about shame experiences, shame is a difficult emotion to detect, especially as it comes in so many disguises.
Generally speaking, in coping with shame we can observe two general strategies:
attacking the self or attacking others. Initially during a shame experience, hostility is directed inward, toward the self (“I’m worthless,” “I’ve never been any good”). Some people, like Steven, go as far as withdrawing from the real world. But in an attempt to feel better about what is experienced as shameful, some people lash out and blame others, showing reactions of avoidance, defensiveness, and denial. Others try to compensate for feelings of shame or unworthiness by attempting to be exceptionally giving; by pleasing others, they hope to improve their feelings of self-worth. Although these various scripts can temporarily help the person feel less ashamed, ultimately they can make matters worse. Without addressing the source of shame, a self-reinforcing negative feedback loop isenacted, through which shame chisels into the core of who the person is.
The Origins of Shame
Given the pervasiveness of this emotion across ages and cultures, what’s the adaptive purpose of shame? From an evolutionary point of view, we could hypothesize that shame has evolved under conditions where survival depended on people abiding by certain norms. They needed to band together to effectively operate as a group to better deal with the terrifying forces of nature. In Paleolithic times, shame would have been the way to establish a group’s pecking order to create the best way of cooperation. It would be an effective mechanism to establish clear dominance-submission rankings. Interestingly, these derivatives of early animalistic behavior patterns can still be observed today when we tend to take a compliant posture out of shame, when we subject ourselves to the power and judgment of others.
From a psychological developmental point of view, shame can be seen as a complex emotional response that humans acquire during early child rearing, when children are completely dependent on the bond with their caregivers. It is a very basic emotion: Children seek to live up to their parent’s expectations, and failing to do so, experience shame. Toddlers exhibit early feelings of embarrassment that can turn into full-blown shame within their first three years of life.
Shame can ultimately serve a purpose if it means that, for example, a toddler feels ashamed after being scolded for running into traffic. Because toddlers’ brains aren’t sophisticated enough to understand that traffic is dangerous, the feeling of shame is enough to keep them from endangering themselves again. But shame is also a horrible feeling. Children who are continually criticized, severely punished, neglected, abandoned, or in other ways mistreated quickly get the message that they are inadequate, inferior, or unworthy. These shameful experiences damage the roots from which self-esteem grows. Such dysfunctional parenting styles can make children shame-bound. This kind of shame is very difficult to overcome. The formative wounds of childhood — scars from being teased, bullied, or ostracized by parents, peers, and others — can become fixed in our identity.
Dealing with Shame
The more powerful our experience of shame, the more we feel compelled to hide those aspects from others, and even from ourselves. The first step is thus to bring to light whatever is seen as shameful. After all, a wound that’s never exposed will never heal. If the wound is deep enough, you may need to ask a counselor or therapist for help. Being able to discover the origins of shame-like experiences will set the stage of having greater control over your life as you become attuned to what triggers these shame reactions.
A second step is to cultivate self-compassion — to embrace who you are and treat yourself in the same respectful, empathetic way you’d treat others. For example, if one of Steven’s friends or direct reports had bombed their presentation, he would have been supportive. “You tried hard, but you let your nerves get the better of you,” he might have said, or “You’ll get better with more practice. Let’s hire a public speaking coach.” When you’re feeling shame, ask yourself: Would I talk to a friend the way I’m talking to myself right now? This question can help you recognize when a negative thought spiral is getting the upper hand, and can challenge your shame-based thinking.
Engaging in these corrective emotional experiences (as they are known in psychology) can help you improve your sense of self-esteem, increase your feelings of worthiness and belonging, foster greater self-acceptance, and reduce unhealthy reactions to shame, such as withdrawal and counterattack.
Shame is part of the human experience. Keeping your feelings of shame in perspective can relieve you of a harmful tendency to self-blame, and, eventually, make peace with your shadow side. Knowing that you are good enough, worthwhile, and deserving of love and acceptance is essential for building resilience and living your most authentic life.
Source: Harvard Business Review: https://hbr.org/2017/06/dont-let-shame-become-a-self-destructive-spiral
Mental health has been described as a “slow-growing epidemic” and the number of people dealing with it has increased by 10 per cent in the last 10 years.
The worst thing about it is that it doesn’t discriminate- anyone can be affected by it.
Check out 51 of the biggest celebrities in showbiz talking about their experiences with mental health, depression or anxiety.
Ryan Reynolds opened up about the anxiety he experienced whilst filming Deadpool. “I never, ever slept. Or I was sleeping at a perfect right angle – just sitting straight, constantly working at the same time”, he explained. “By the time we were in post [production], we’d been to Comic-Con, and people went crazy for it. The expectations were eating me alive.” The 40-year-old credited his wife, Blake Lively, for helping him through it: “Blake helped me through that. I’m lucky to have her around just to keep me sane”.
Will Young
When Will Young pulled out of Strictly Come Dancing insiders said it was a result of his anxiety. He has always been honest about battling his demons. The singer said: “It’s very isolating. There’s a part of my brain that is telling me that you’re about to die, you either shut down, freeze or you run. The only thing I can do is go to bed.” He added: “There have been dreadful times where I’ve been suicidal and on the floor.”
Lena Dunham
Lena Dunham posted a message on her Instagram about using exercise to deal with her anxiety. She wrote: “Promised myself I would not let exercise be the first thing to go by the wayside when I got busy with Girls Season 5 and here is why: it has helped me with my anxiety in ways I’ve never dreamed possible. “To those struggling with anxiety, OCD, depression: I know it’s mad annoying when people tell you to exercise, and it took me about 16 medicated years to listen. I’m glad I did. It ain’t about the ass, it’s about the brain.”
Demi Lovato
The singer has never shied away from opening up about her problems and is determined to de-stigmatise mental illness by sharing her story. Demi Lovato said: “I just think mental illness is something people need to learn more about.I want people to know it’s okay to ask for help and it’s okay to have a mental illness.” Speaking at the National Council for Behavioral Health in Washington DC, she said: “I think it’s important that people no longer look at mental illness as something taboo to talk about. It’s something that’s extremely common, one in five adults has a mental illness, so basically everyone is essentially connected to this problem and this epidemic,” she explains. “The problem with mental illness is people don’t look at it as a physical illness. When you think about it, the brain is actually the most complex organ in your body. We need to treat it like a physical illness and take it seriously.”
James Arthur
James Arthur might be the comeback kid but he has spoken about going through dark times in the past. The X Factor considered taking his life after being dropped from Simon Cowell’s record label in 2013. He said: “If I was ever near a balcony, or in my car, I’d have an image of me jumping over or driving off the road. “But then I’d think, ‘Don’t do it, you’ve got sisters, you’re the man of the family.’ But there was many a time I thought of it.”
Kerry Washington
As Scandal’s Olivia Pope, she is always solving problems and Kerry Washington knows the importance of having therapy to sort her own life too. “My brain and my heart are really important to me. I don’t know why I wouldn’t seek help to have those things be as healthy as my teeth. I go to the dentist. SO why wouldn’t I go to a shrink?”
Wentworth Miller
Wentworth Miller, has spoken candidly about coming out and considering suicide.
The Prison Break actor said: “I would say what others have said: ‘it gets better. One day, you’ll find your tribe. You just have to trust that people are out there waiting to love you and celebrate you for who you are.”In the meantime, the reality is you might have to be your own tribe. You might have to be your own best friend. That’s not something they are going to teach you in school. So start the work of loving yourself.”
Cara Delevingne
She is one of the most successful models in the world but Cara Delevingne used her power for good when she posted on Twitter about her battle with depression.
She Tweeted: “I suffer from depression and was a model during a particularly rough patch of self hatred. I am so lucky for the work I get to do but I used to work to try and escape and just ended up completely exhausting myself. I am focusing on filming and trying to learn not to pick apart my every flaw. I am really good at that.”
Sarah Silverman
Sarah Silverman explained: “People use ‘panic attack’ very casually out here in Los Angeles, but I don’t think most of them really know what it is. Every breath is laboured. You are dying. You are going to die. It’s terrifying. And then when the attack is over, the depression is still there.
“I wouldn’t wish depression on anyone. But if you ever experience it, or are experiencing it right now, just know that on the other side, the little joys in life will be that much sweeter. The tough times, the days when you’re just a ball on the floor-they’ll pass. You’re playing the long game and life is totally worth it.”
Justin Bieber
Justin Bieber spoke to NME about how fame had a negative effect on his mental health: “I’m struggling just to get through the days. I think a lot of people are
This life can rip you apart. [I get depressed] all the time. And I feel isolated. You’re in your hotel room and there are fans all around, paparazzi following you everywhere, and it gets intense. When you can’t go anywhere or do anything alone you get depressed. I would not wish this upon anyone.”
Amanda Seyfried
Amanda Seyfried talked to Glamour about receiving therapy for her anxiety: “I still do get terribly nervous, and that’s partly due to the fact I think too much and overanalyse things. I’ll start worrying about my parents or my dog, and I’ll picture him opening the window of my apartment and falling out, even though I can’t get that thing open myself.”
Kristen Stewart
“Between ages 15 and 20, it was really intense. I was constantly anxious. I was kind of a control freak. If I didn’t know how something was going to turn out, I would make myself ill, or just be locked up or inhibited in a way that was really debilitating,” Kristen Stewart talks about not being able to let go.
Colin Farrell
Colin Farrell spent six weeks in a rehabilitation centre to treat his depression and drug and alcohol addictions in 2005. The 40-year-old told Friday Night With Jonathan Ross: “Desperation will allow you to do incredible things in the name of survival…I had created an environment for myself, a way of living for myself which, on the outside, seemed incredibly gregarious and vivacious. “I don’ believe I have any chemical predisposition towards depression, but let’s just call it… I was suffering from a spiritual malady for years and I induldged it.”
Zoella
Zoella never shies away from discussing what it’s like to deal with anxiety. When the vlogger posted a video about her panic attacks, it got over 3.5 million views.
Writing for Glamour , she said: “I go through phases where my anxiety isn’t as bad and when it’s pretty awful. When it’s good, I’ll be able to leave the house, go shopping, visit other countries for work, do meet and greets and generally live life like a ‘normal person’. When it’s bad, I can’t even leave my bed or I’ll start my day off by opening my eyes and having a panic attack.”
Zayn Malik
The One Direction star has been praised for his honesty over his “extreme anxiety” which has led to him having to cancel concerts. Zayn Malik said: “I have been working over the last three months to overcome my extreme anxiety around major live solo performances.
“I don’t have it in me to feel secure in anything I do. I always strive towards something better.
“It’s why I sometimes come across the wrong way – a bit distant. I’m stressed out trying to control how I’m perceived.”
Nicole Scherzinger
The X Factor judge opened up about her battle of bulimia calling it “a horrible, paralysing disease”. Nicole Scherzinger said:
“I had started losing my voice, I couldn’t sing at shows, and then I remember my manager finding me passed out on the floor in Malta or in the south of France. I thought, ‘I’m going to lose everything I love if I don’t love myself.’ … It’s sad to see how I wasted my life. I had such a great life on the outside, the [Pussycat] Dolls were on top of the world, but I was miserable on the inside. I’m never letting that happen again; you only get one life – I was 27 only once.”
Ruby Rose
Ruby Rose talked about her struggles with depression after a fan found an old Tweet she posted in 2013.
It said: “It is with great sadness that despite everything I’ve tried in a short time I was given I am losing my battle with depression.”
Ruby took to Instagram to explain the difficult period in her life: “I had hit a rock bottom.”
After moving to America and a stint in rehab, the actress got her life back on track.
She added: “It just makes me wonder how many others are days, hours, seconds away from realising their worth, their potential? And once the dark cloud is lifted will be truly happy and free.”
Winona Ryder
Winona Ryder explains how depression feels: “You can’t pay enough money to cure that feeling of being broken and confused. It’s not like every day’s been great ever since. You have good days and bad days, and depression’s something that, y’know, is always with you.”
Zosia Mamet
The Girls star spoke to Glamour about how she had been dealing with an easting disorder since she was a child. Zosia Mamet said: “I’m an addict in recovery. We need to treat eating disorders just as seriously as other addictions. I’m not fat; I’ve never been fat. But ever since then, there has been a monster in my brain that tells me I am. During treatment, I discovered that my disorder has never really been about weight , or food – that’s just the way the monster manifests itself. Really these diseases are about control: control of your life and of your body.”
Adele
“I have anxiety attacks, constant panicking on stage, my heart feels like it’s going to explode because I never feel like I’m going to deliver, ever,” Adele reveals.
Beyonce
Even a megastar like Beyonce sometimes struggles to feel ok.
She said: “It was beginning to get fuzzy – I couldn’t even tell which day or which city I was at. I would sit there at ceremonies and they would give me an award and I was just thinking about the next performance. My mother was very persistent and she kept saying that I had to take care of my mental health.”
Catherine Zeta-Jones
Catherine Zeta-Jones disappeared from the spotlight to deal with her bipolar disorder but decided to talk about it to help others in similar positions.
She said: “I never wanted to be as open about it as I was. I have a British stiff-upper-lip mentality. I’m not the kind of person who likes to shout out my personal issues from the rooftops but, with my bipolar becoming public, I hope fellow sufferers will know it is completely controllable. I hope I can help remove any stigma attached to it, and that those who don’t have it under control will seek help with all that is available to treat it. If I’ve helped anybody by discussing bipolar or depression, that’s great.”
Christina Ricci
Former child star Christina Ricci
opened up about how her fame affected her recovery from anorexia.
“Somebody actually found out about it and outed [me] while I was recovering,” she explained. “It was a horrifying thing to do to a 14-year-old trying to cope with a devastating illness. And, out of rage, I vowed that no one would ever be able to out me for a secret again. So I was going to be completely honest in the rest of my life. I don’t want to be hurt in that way again.”
Dakota Johnson
The Fifty Shades of Grey actress admitted she struggles with anxiety going to auditions for parts. Dakota Johnson
said: “Sometimes I panic to the point here I don’t know what I’m thinking or doing. I have a full anxiety attack.”
Ellen DeGeneres
The talkshow host has spoken about the anger and depression that she faced after she came out. Ellen DeGeneres
told Mail On Sunday : “When I walked out of the studio after five years of working so hard, knowing I had been treated so disrespectfully for no other reason than I was gay, I just went into this deep, deep depression.
“It’s so corny but it’s true. You have no idea where the darkest times of your life might end, so you have to just keep going.”
Ellie Goulding
“It was the weirdest time of my life.” revealed Ellie Goulding. “Sick, horrible things would go through my mind but I didn’t want to draw attention to myself. I was sceptical [about having cognitive behavioural therapy] at first because I’d never had therapy, but not being able to leave the house [because of panic attacks] was so debilitating. And this was when my career was really taking off… My surroundings would trigger a panic attack, so I couldn’t go to the studio unless I was lying down in the car with a pillow over my face. I used to beat myself up about it. There were a couple of times after I released Delirium when I was doing promo and thought, ‘Oh god, it’s coming back, it’s coming back,’ but it didn’t. I think my body has become quite good at controlling anxiety.”
Emma Stone
“The first time I had a panic attack I was sitting in my friend’s house, and I thought the house was burning down. I called my mom and she brought me home, and for the next three years it just would not stop.
“I would ask my mom to tell me exactly how the day was going to be, then ask again 30 seconds later. I just needed to know that no one was going to die and nothing was going to change,” Emma Stone tells the The Wall Street Journal.
Frankie Bridge
The Saturdays star bravely opened up to Glamour in 2012 about her eight-year long secret battle with depression. Frankie Bridge revealed: “One night, I got upset because Wayne (Bridge, her husband) hadn’t bought the right yoghurts; I managed to convince myself that he didn’t know me at all. It set off this spiral of negative thinking – that if I disappeared, it wouldn’t matter to anyone. In fact, it would make everybody’s life easier. I felt that I was worthless, that I was ugly, that I didn’t deserve anything.”
It lead To Frankie going to hospital to get treatment and helped her get it under control.
She added: “Nine times out of ten, my depression is under control. I get a bit emotional to think I felt so low about myself, that I shouldn’t be around people I love, because I can’t make them happy. I did lose myself, but I feel like me again now.”
Glenn Close
The actress is so passionate about getting people talking about mental illness that she founded Bring Change 2 Mind in 2010 with her sister, Jessie. Glenn Close
revealed to Mashable she was diagnosed with depression in 2008.
She said: “I never realised that maybe I could get a little help. We’re talking about her own experience with depression, an illness she was diagnosed with only eight years ago.
It was truly a surprise.”
For years, the Hollywood legend thought she probably had Attention Deficit Disorder, which can cause hyperactivity, impulsiveness or problems with concentration.
“I felt this inertia that would come over me,” she says. “You think of something and it just seems too much, too hard. That’s how it manifested in me.”
Halle Berry
Halle Berry talked about her lowest point:
“I was sitting in my car, and I knew the gas was coming when I had an image of my mother finding me. She sacrificed so much for her children, and to end my life would be an incredibly selfish thing to do. My sense of worth was so low. I had to reprogram myself to see the good in me. Because someone didn’t love me didn’t mean I was unlovable. That’s what the break-up of my marriage reduced me to. It took away my self-esteem. It beat me down to the lowest of lows.”
Hayden Panettiere
Hayden Panettiere opened up about her postpartum depression on Live! With Kelly and Michael
She said: “It’s something a lot of women experience. When [you hear] about postpartum depression you think it’s ‘I feel negative feelings towards my child, I want to hurt my child. I’ve never, ever had those feelings. Some women do. But you don’t realise how broad of a spectrum you can really experience that on. It’s something that needs to be talked about. Women need to know that they’re not alone, and that it does heal.”
She continued: “It’s something that’s completely uncontrollable. It’s really painful and it’s really scary and women need a lot of support. There’s a lot of misunderstanding. There’s a lot of people out there that think it’s not real, that it’s not true, that it’s something that’s made up in their minds, that ‘Oh, it’s hormones.’ They brush it off.”
J.K. Rowling
J.K. Rowling has never shied away from speaking out and raising awareness on depression.
The Harry Potter writer said: “What’s to be ashamed of? I went through a really rough time, and I am quite proud that I got out of that,” she told a student journalist in 2008.
She has also been a source of hope for many in difficult moments through the famous Dumbledore quote, “Happiness can be found even in the darkest times if one only remembers to turn on the light.”
Kate Moss
She’s the most successful supermodel in the world but Kate Moss suffered from anxiety when she was starting out in the fashion world.
She said: “I had a nervous breakdown when I was 17 or 18, when I had to go and work with Marky Mark and Herb Ritts. It didn’t feel like me at all. I felt really bad about straddling this buff guy. I didn’t like it. I couldn’t get out of bed for two weeks. I thought I was going to die.”
David Beckham
David Beckham attempted to de-stigmatize Obsessive Compulsive Disorder by speaking out about how he deals with his condition.
He said: “I’ve got this Obsessive Compulsive Disorder where I have to have everything in a straight line or everything has to be in pairs. I’ll put my Pepsi cans in the fridge and if there’s one too many then I’ll put it in another cupboard somewhere.
The father of four added: “I’ll go into a hotel room. Before I can relax I have to move all the leaflets and all the books and put them in a drawer. Everything has to be perfect.”
Oprah Winfrey
The chatshow host seems to have the world at her feet but Oprah Winfrey revealed in a chat with Access Hollywood about her anxiety while filming The Butler.
She said: “I remember closing my eyes in between each page because looking at the page and the words at the same time was too much stimulaton for my brain.”
Pete Wentz
The Fall Out Boy bassist has always been candid about his mental health struggles. Pete Wentz, who was diagnosed with manic-depression said: “I think I went through when I was in my 20s… I went through a lot of highs and lows. For me… you’re travelling on the road. Everything is available to you and you can get what you need to get, or not… People just want to keep the machine going. They don’t so much care how healthy you are.”
The father of two, who describes his children as the “ultimate happy pill” added: “ My highs, my happiness are really high and my lows are very low and I’m not able to regulate between the two. Through actual therapy and having kids it’s way more under control and something I can see when I’m on the roller coaster and control it more.”
Nadiya Hussain
The 2015 Great British Bake Off winner explains how she copes with her anxiety disorder.
Speaking on Loose Women, Nadiya Hussain said: “When I was doing Bake Off it was quite stressful and I had a little elastic band across my hand. I would ping it and forget why I was worried, I would use that in Bake Off but in week five or six it pinged off.”
Melanie C
Mel C
revealed falling pregnant with her daughter, Scarlett helped her recover from her eating disorder.
She said: “When I was in the Spice Girls, the stress of suddenly being thrust into the limelight led me into an unhealthy relationship with food and exercise. I became obsessed about what I ate and I cut lots of food groups, like carbs and protein, out of my diet. I survived on fruit and vegetables and little else … I had to be healthy and from the moment I knew I was pregnant, I wanted to give Scarlet the nutrition she needed to grow fit, strong and healthy.”
Miley Cyrus
The former Disney star prides herself on her honesty. Miley Cyrus said: “I went through a time where I was really depressed. I locked myself in my room and my dad had to break my door down. My fans know that I’ve struggled with depression, and that helped them get over theirs. That gives me a big purpose – a reason to wake up in the morning that’s bigger than to put my f**king feathers and my little outfit.”
Lucy Spraggan
Lucy Spraggan
, who was a contestant alongside Rylan Clark and James Arthur on 2012 X Factor, has revealed her witty songs are inspired by her personal battle with mental health issues.
The 25-year-old singer has struggled with depression, anxiety and paranoia and she even contemplated killing herself.
She said: “My anxiety got quite bad and it got to a point where when people stopped me to say hello, which I usually always loved, I couldn’t keep up a façade. I had to find a person I felt comfortable telling so I spoke to a therapist.”
Leonardo DiCaprio
Leonardo DiCaprio talks about dealing with OCD at work.
He said: “I remember my makeup artist and assistant walking me to the set [of ‘The Aviator’] and going, ‘Oh God, we’re going to need 10 minutes to get him there because he has to walk back and step on that thing, touch the door and walk in and out again.”
Lady Gaga
Lady Gaga reveals: “I was angry, cynical and had this deep sadness like an anchor dragging everywhere I go. I just didn’t feel like fighting anymore. I didn’t feel like standing up for myself one more time – to one more person who lied to me. I really felt like I was dying – my light completely out. I said to myself, ‘Whatever is left in there, even just one light molecule, you will find it and make it multiply. You have to for you. You have to for your music. You have to for your fans and your family.’”
Taylor Swift
“And it can feel, at times, if you let your anxiety get the better of you, like everybody’s waiting for you to really mess up – and then you’ll be done,” Taylor Swift speaks out about her struggles.
Carrie Fisher
The Star Wars actress has suffered from bipolar disorder for years and is still treated for it today. Carrie Fisher said: “Sometimes you didn’t want to be that person. You didn’t want to hold the dinner party hostage. And I didn’t have a choice. I’d keep people on the phone for eight hours. When my mania is going strong, it’s a sort of clear path. You know, I’m flying high up onto the mountain, but it’s starts too fast. I stop being able to connect. My sentences don’t make sense. I’m not tracking anymore and I can’t sleep and I’m not reliable.”
Jennifer Lawrence
Jennifer Lawrence spoke out about her anxiety as a child: “When my mother told me about my childhood, she always told me that there was a light in me, a spark that inspired me constantly. When I started school, the light went out. It was never known what it was, a kind of social anxiety.”
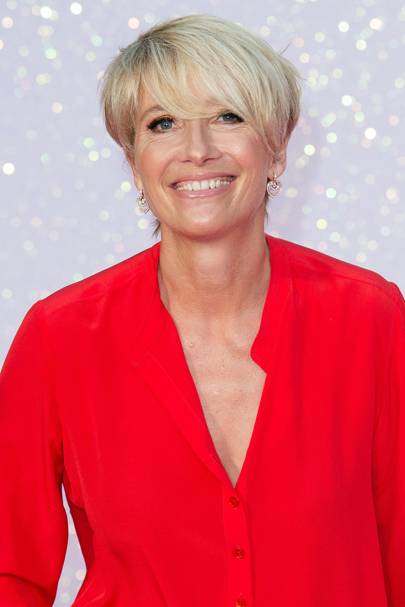
Emma Thompson
Emma Thompson opened up about her battle with depression in 2010 on Radio 4’s Desert Island Discs .The Oscar-winning actress admitted the condition had crippled her most of her life. She first suffered while playing the lead role in a West End revival of the musical, Me and My Girl in the 1980s.
She said: “I think my first bout of that was when I was doing Me and My Girl, funnily enough.
“I really didn’t change my clothes or answer the phone, but went into the theatre every night and was cheerful and sang the Lambeth Walk. That’s what actors do. But I think that was my first bout with an actual clinical depression.”
The 55-year-old admitted it was work that helped her get better and also meeting her husband, Greg Wise on set of Sense and Sensibility.
She said: “The only thing I could do was write. I used to crawl from the bedroom to the computer and just sit and write, and then I was alright, because I was not present.
“Sense and Sensibility really saved me from going under, I think, in a very nasty way.”
Kate Winslet
Kate Winslet talked about the weight loss addiction she developed as a teenager, and has admitted to starving herself in order to win acting roles: “When I was 15, I was nearly 14 stone. I was uncomfortable and self-conscious. I knew I wanted to be an actress and was big. Over a year I sensibly got down to 10 stone. Then I became addicted to losing weight and went too far. I was never anorexic or bulimic.”I went through a three-month experimental laxative time, which was absolutely awful. Luckily I was strong enough to be able to say to myself, ‘What are you doing? You are just really hungry.’ The whole weight thing drives me crazy. This stuff is so important to me because I have been there and know what a vicious cycle it is.”
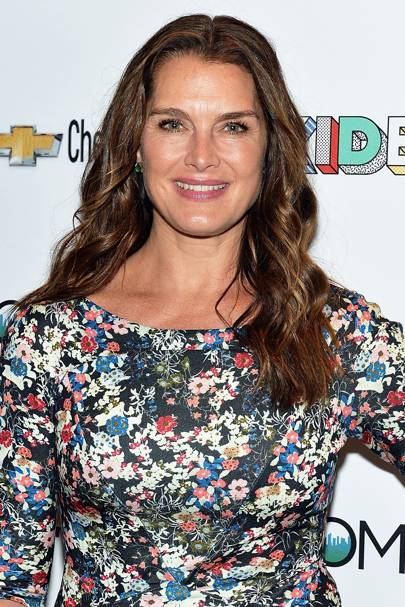
Brooke Shields
Brooke Shields spoke about her postpartum depression after the birth of her daughter in 2003.
She said at one point she “didn’t want to live anymore” but she sought treatment and managed to bring her disorder under control
“If I had been diagnosed with any other disease, I would have run to get help. I would have worn it like a badge. I didn’t at first—but finally I did fight. I survived.”
Drew Barrymore
The actress rose to fame appearing in ET when she was just seven but by the time she was a teenager, she was already addicted to drugs and alcohol and attempted suicide cutting her wrists when she was just 13.
Speaking in 2015 to the Guardian, Drew Barrymore said: “I really had a fear that I was going to die at 25. And half yes, because no matter how dark shit got, I always had a sense that there should be goodness. I never went all the way into darkness. There were so many things I could have done that would have pushed me over the edge and I just knew not to go there.”
Gwyneth Paltrow
“When my son, Moses, came into the world in 2006, I expected to have another period of euphoria following his birth, much the way I had when my daughter was born two years earlier. Instead I was confronted with one of the darkest and most painfully debilitating chapters of my life.” Gwyneth Paltrow opens up with dealing with postpartum depression
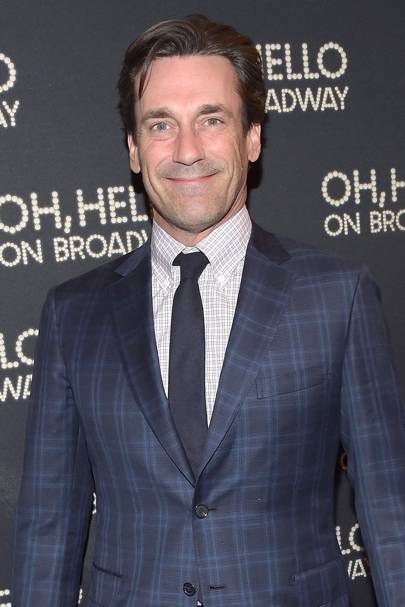
Jon Hamm
“Honestly? Antidepressants help! If you can change your brain chemistry enough to think: ‘I want to get up in the morning; I don’t want to sleep until four in the afternoon. I want to get up and go do my shit and go to work’. Reset the auto-meter, kick start the engine,” Jon Hamm speaks frankly about getting help.
Kesha
Kesha penned an open letter about her experiences in an eating disorder rehabilitation centre.
“I’ve always tried to be a crusader for loving yourself, but I’d been finding it harder and harder to do personally. I felt like part of my job was to be as skinny as possible, and to make that happen, I had been abusing my body. I just wasn’t giving it the energy it needed to keep me healthy and strong. My brain told me to just suck it up and press on, but in my heart I knew that something had to change. So I made the decision to practice what I preach. I put my career on hold and sought treatment. I had to learn to treat my body with respect.”
Louise Pentland
YouTube star, Louise Pentland aka Sprinkle of Glitter,
explains how counselling helped cure her anxiety.
She said: “Over the past few years I’ve experienced horrible bouts of anxiety. When that moment hits, my whole body tenses up and my mind spirals, thinking the worst – that I’m not safe and can’t get home. I start crying, my breathing is all over the place and, in extreme cases, I throw up.
“Everything came to a head last November, after my marriage ended. Life suddenly felt so different – and hard. I had a terrifying panic attack at home. Everything came to a head last November, after my marriage ended. Life suddenly felt so different – and hard. I had a terrifying panic attack at home.”
Olivia Munn
The X-Men: Apocalypse star suffers from social anxiety and trichotillomania, which is the obsessive compulsion to pull out your own hair. Olivia Munn told New York Daily News: “I don’t bite my nails, but I rip out my eyelashes. It doesn’t hurt, but it’s really annoying. Every time I run out of the house, I have to stop and pick up a whole set of fake eyelashes.”
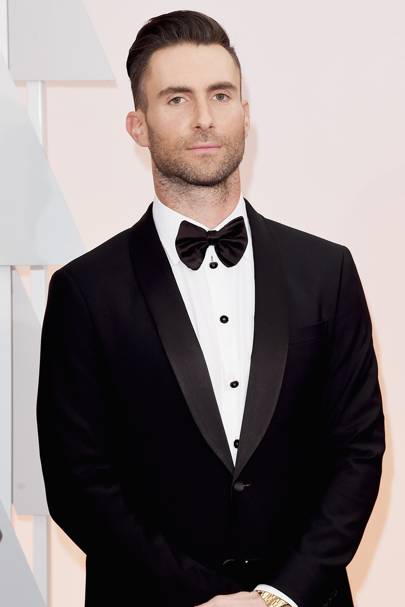
Adam Levine
Adam Levine, frontman of Maroon 5 explained: “When I was first diagnosed with ADHD, it wasn’t a surprise because I had difficulty in high school focusing. And I think now, people notice my ADHD as an adult on a daily basis. When I can’t pay attention, I really can’t pay attention.”
I previously shared my truth about my battle with depression and self-injury in a piece I wrote titled “An Open Letter to Black Women About Mental Health.” Not only did I openly share my experiences with depression, but I urged other black women to break away from the cultural stigma surrounding mental illness, to rid themselves of the weight that comes with carrying the “strong black woman” title and to seek professional treatment for their struggles.
I took some time out to re-read my letter, and I realized that there is a fundamental piece that was missing. When I wrote it, I felt as if I were hitting the nail on the head, but I wasn’t focused on the foundation that nail was going into. If I am going to address a community to seek professional help, I need to address those who drive the mental health care system to understand how to tend to — as well as make themselves available to — this particular community.
There are so many folks living behind the looking glass who fail to recognize or comprehend the contemporary social problems that people from minority backgrounds encounter just for being human — racism, prejudice, discrimination, criminalization and deep-seated cultural stereotypes, to name a few. These collective societal issues are just as detrimental to our well-being as the “strong black woman” supposition, and such matters are linked to the prevalence of mental illness, particularly trauma, within minority and African-American communities.
As a woman who identifies as African-American and was once diagnosed with severe depression, I experienced several personal barriers to treatment not solely due to shame and stigma, but also due to my lack of knowledge around mental health, the lack of African-American treatment providers within the mental health scope, and most importantly, the cost of mental health services. Studies show that African-American patients are more likely to pursue African-American providers, as their commonality in regards to race helps to create a therapeutic relationship where the client feels accepted and understood, and the provider is more attune to culturally sensitive issues. This cultural match between patient and provider also leads towards a greater outcome for the development and successful completion of treatment goals and greater interactive sessions.
Studies show that nearly one-fourth of African Americans are uninsured, a percentage 1.5 times greater than the white rate. The average private provider (clinical social workers, psychiatrist, and psychologist) charges between $60-$300 per 45-minute session and works primarily out-of-network. Furthermore, providers typically recommend or mandate weekly sessions to ensure a rapport is continuously being built and so that they can better examine whether the services are proving to be effective for the client. On a monthly basis, mental health treatment alone can accrue an out-of-pocket cost between $120-$1,200.
When a private practitioner sets a rate for $200 for a therapy session, it is easily discernible who his or her target clientele will be. Yes, therapy can serve as a healthy outlet to processing emotions and thus, requires extreme care and attention to the needs of others, but it also takes extreme vulnerability, and when it costs someone that much to be vulnerable, it is simply a privilege that most people in need of mental health services cannot afford.
Providing culturally responsive treatment requires not just being aware of one’s biases and judgments or negative attitudes towards race and cultural stereotypes, but also knowing and understanding the individuals who need access to treatment and choosing to make yourself available to address the needs of those who may come from oppressed or marginalized groups by providing affordable care.
There is also a greater need to increase diversity among mental health providers. Training more African-American mental health workers may decrease the mental health gap correlated to stigma and lack of educational awareness, but this would also require getting to the core of the inadequate educational opportunities available for African-Americans along with the low college acceptance rates and the cost of tuition, which serves as barriers to gaining professional opportunities.
As a social worker myself, I got into this field knowing that this is not a lucrative venture, and I believe there should not be a monetary value placed on the quality of care that an individual receives based on their socio-economical and racial background. The health care system was built to serve the underserved and examine social injustice, yet there are still barriers set in place for those this system was designed for.
As much as I strongly encourage black women (and also black men) to seek professional care and to not be ashamed to be in need of help, I equally strongly ask and encourage the systems at play to provide greater access to the professional care that we need. If we are going to hit the nail on the head, lets make sure it’s not going directly into the coffin.
Patients with Pseudodysphagia complaint about the inability to swallow but they do not have any physical symptoms to account for their condition. The word Pseudodysphagia comes from GreekPhagophobia where “phagein” means eating and “phobos” means deep dread, aversion or fear. Other names for this phobia include sitophobiawhere sito is Greek for food.
Pseudodysphagia is an unnatural and irrational fear of choking or swallowing that causes a person to believe s/he will become ill or die if one tries to eat solid foods. The nature of difficulty these patients face when it comes to swallowing varies depending on the level of their fear: some people can only eat very small pieces of well lubricated foods, while others are afraid of drinking liquids or swallowing pills or tablets. Naturally, there is substantial loss of weight in this phobia and it is a debilitating condition that can interfere with one’s day-to-day life.
What are the causes of fear of choking phobia?
As with most specific phobias, Pseudodysphagia also begins with a negative experience related to swallowing food. As a child, the phobic might have choked, vomited or had an “embarrassing response” after swallowing certain types of foods. The brain then creates the same response as a defensive mechanism each time one is confronted with the thought of eating. For example, a patient recalls choking (as a child) on a quarter after it got lodged in his throat. He lost consciousness and turned blue and recalls fearing eating solid foods like steaks, meats, capsules, pills (anything hard or chewy) after the incident.
Psychiatrists also believe that most people with the extreme fear of choking are usually anxious or suffering from other psychiatric disorders like depression, Hypochondriasis, Agoraphobia or have a general predisposition to panic attacks.
The fear of choking is also often listed in conjunction with Globus sensation-(a condition that comes and goes wherein the patient feels there is a lump in his throat that prevents him from eating). However, the two conditions are different; Globus sensation is more common and occurs when patients are typically suffering from ear-nose-throat infections that cause them to fear they might choke or vomit after eating.
Symptoms of Pseudodysphagia
Psychogenic Dysphagia leads to many psychological symptoms, the most important one being inefficient ordisorganizedswallowing. Other symptoms of the fear of choking include:
Avoidance of food, especially swallowing pills, tablets, hard and chewy foods
Abnormal oral behavior is also seen including deviant tongue movements, feeling the throat pressure, and complaint of globus sensation.
Malnutrition and weight loss are common side effects of this phobia
General difficulties in breathing, swallowing and other issues like elevated heart rate, feeling dizzy, having fearful thoughts of dying, passing out or embarrassing oneself in front of others are common symptoms of Pseudodysphagia.
Nightmares about choking on candy, peanuts or indelible objects also tend to keep these patients awake at night.
Some refuse to eat in front of others thinking that swallowing makes “unpleasant noises”.
Needless to say, this phobia is a debilitating condition that affects the normal life of the patients.
Would you describe your life with your significant other as a routine? Nothing is more boring than monotony. Here’s five easy ways to give your relationship a little OOMPH!
1. Make time for each other.
Absence is rumored to make the heart grow fonder, but that doesn’t mean your relationship can thrive without any time devoted to it. Life gets busy, especially if you have kids/school/a job/a second job and OMG, ALL THE THINGS; but your relationship is a priority no matter how full your plate may be. Have a daily, 10-minute mini-date where you snuggle up with a silly YouTube video, take a quick walk, have some ice cream, or whatever you both enjoy.
2. Switch up date-night.
Dinner-and-a-movie is a staple for a reason (because it’s fun), but it can grow stale without the occasional mix-up. For example: You could grab coffee or hot cocoa, go to a park on a breezy day and find yourself with a perfect excuse to cuddle.
3. Take an adventure.
Do something exciting together! You could take a cruise, go on a road-trip, jump out of a plane, visit a rain forest, or climb Mt. Everest.
4. Learn something new.
Tackle a hobby of mutual interest with your partner. Whether you want to learn to speak Italian, become a Jeopardy contestant or create handmade jewelry is up to you. Challenging yourselves to grow will strengthen your bond and shake-up your ho-hum love life.
5. Create a Bucket List.
Make a list of all the crazy, ambitious, and wonderful things you want to do with your partner. Be happy you have someone to share your life with. Take small steps to make your Bucket List items happen.
ANGRY?
There is no reason to bottle up our feelings in relationships. I know you might be intimidated by conflict, but there is no hiding from it. Sure, you could just keep saying “nothing is wrong,” but that would only delay the inevitable. Feelings that are held in have a way of intensifying. Pissed off? Take a deep breath and let’s deal with it:
6. Count to 10.
If you find word vomit escaping your lips, one of those hurtful things you know you’re going to regret saying later, hold it in and count to ten. Breathe in. Breathe out. Still want to say it? Go for it. Not so much? Crisis averted.
7. See it from the other side.
“It was a great surprise to me when I discovered that most of the ugliness I saw in others, was but a reflection of my own nature.” -Anonymous
Before you criticize another person, take a second to look at the scenario from their perspective. Most people act the way they do for a reason. See yourself in their eyes to make sure the problem doesn’t reside in yourself.
8. Give and receive.
Did you get a wonderful back rub after a rough day at the office? Return the favor (or surprise your partner with a tasty dessert or coffee at work). A perceived imbalance in who puts the most into your relationship can make a person upset in a hurry. Split chores and housework fairly, take turns deciding what to have for dinner, and aim for equality in your relationship.
9. Express yourself with no filter.
You can’t expect your partner to know something is wrong if you don’t tell them. Express your feelings without filter (especially if you’re being asked “What’s wrong?” repeatedly). Confrontation isn’t fun but it’s also unavoidable. Dragging out a fight is just going to place unnecessary strain on your relationship, so get it over with and express yourself.
10. Appreciate each other.
What do you find sexy or handsome about your partner? Do they have any quirks you find wonderful? What is the sweetest thing they ever did for you? Sometimes, we’re so busy focusing on our partner’s negative traits that we forget to appreciate what we have and what made us fall in love with them in the first place.
Well, it might not feel like it when you’re in the middle of perimenopause, but the answer is yes. Yes, there is life after menopause – and it’s not so bad.
A reader shared with me recently the grief and emotional struggles she is experiencing as she comes to terms with the fact that she is no longer (at least in her mind) an attractive, desirable woman, since she began to go through perimenopause.
Having walked that road, I know exactly how she feels, and the kinds of questions she is likely asking herself about this profound, mid-life transition called menopause. I mean, let’s face it. You’ve spent 40-something years defining and cultivating a life and personal identity, only to have it obliterated all to hell and back by hot flashes, mood swings, and night sweats.
And that’s just the short list.
But life transitions aren’t easy for anybody. I have a 22 year old son who often laments the loss of his carefree childhood as he is now dealing with grown-up realities like expensive car repairs, health insurance costs, college loan debt, and just the day-to-day, non-sexy, no-fun decisions, grown-ups have to make every day of their life.
I don’t have the heart to tell him that just when he gets this part of his life figured out, it changes all over again.
I think what makes the menopause transition so difficult for women is that we are beginning to face the reality of our own mortality. Sure, we talk about our sagging breasts, our lagging libido, and feeling so oldwhen we start going through perimenopause and menopause. But, what we really mean, is that we realize we are closer to death and dying than we’ve ever been before – and it’s scary. It’s sobering. It’s existential.
But, there’s a funny thing about facing death and dying. It makes you realize how much you should live.
Perhaps that is why many women become so fierce once they reach menopause. They realize without equivocation that the number of years they have left on this earth are ticking down fast, and if they don’t get on with living them they are gone.
The thing I personally love about menopause is that it forces your hand. There’s no place to run, no place to hide. You’re past middle-age and you’re facing down death whether you like it or not. It’s crunch time. Yes, it’s uncomfortable and difficult. Sometimes it’s damn well excruciating. But it’s a crossroad of life, and you get to choose the road you’re going to walk.
I don’t know about you, but I find that rather empowering. I can’t control the fact that I’m dying. But I can control how I live. I don’t have to “go gentle into that good night” so I won’t. I don’t know that I want to“rage, rage, against the dying of the light” either. I had enough of raging and mood swings during perimenopause, thank you very much.
I would much rather just “live like I am dying.” Because we all are, menopause sisters. We all are.
Magnolia Miller is a certified healthcare consumer advocate in women’s health and a women’s freelance health writer and blogger at The Perimenopause Blog.